-

ISTJ Personality Type: Misconceptions, Traits, Relationships, Careers and Scientific Perspective
What is an ISTJ? ISTJ is one of the sixteen personality types described by the Myers-Briggs Type Indicator (MBTI). These individuals with the ISTJ personality type tend to prefer situations and decisions which they have experienced before and usually use a logic-driven approach to predict events, problems or outcomes. Due to this, they can appear…
-

The Hero Who Couldn’t Come Home: A Clinical Reading of Nolan’s Odyssey
Christopher Nolan’s The Odyssey is being read as a film about PTSD. A closer look suggests the wound at its center is moral injury, and that Athena, who wears the face of a girl Odysseus watched his men kill, is guilt made visible.
-

The 2026 Guide to State & Local Mental Health Helplines in California
Unlike Texas, California is anchored by a single, easy-to-remember statewide number. If you need mental health support in California, you can call or text 988 from anywhere in the state to reach the Suicide & Crisis Lifeline, or reach out directly to your county’s dedicated access line below for local, ongoing care. Statewide California Helplines…
-
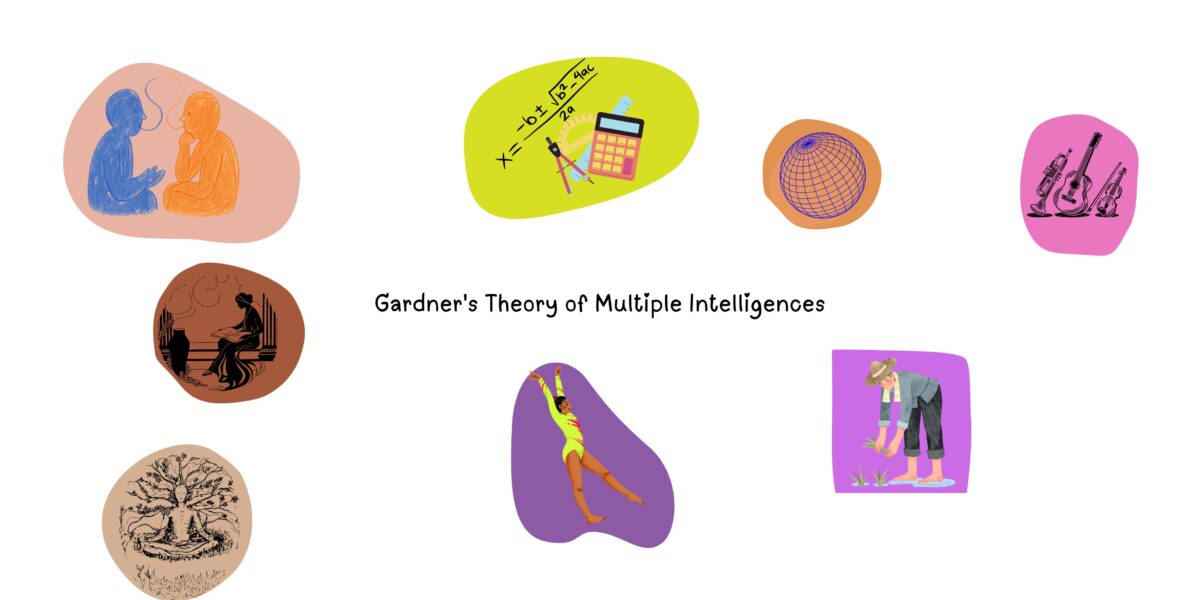
Gardner’s Theory of Multiple Intelligences: Types, Strengths, Weaknesses, and Educational Implications
Howard Gardner (1983) introduced the Theory of Multiple Intelligences (MI) in Frames of Mind: The Theory of Multiple Intelligences. Through this radically new way of seeing intelligence, Gardner challenged the traditional view that intelligence is a single, measurable ability reflected by IQ tests. Instead, he sought to explain the wide variety of human talents observed…
-
Why Do People Become Narcissists? What Psychology Says About the Development of Narcissism
People often ask whether narcissists are born or made, whether poor parenting is to blame, or whether traumatic experiences create narcissistic personalities. The complete story, however, is more complicated than that. The Short Answer:Modern psychological research suggests that narcissism does not develop because of a single event or cause. Instead, it appears to emerge through…
-

How Light Yagami Manipulates People: His Tactics Explained
Few fictional characters are as widely regarded for their manipulative abilities as Light Yagami. Throughout Death Note, he deceives seasoned detectives, evades international law enforcement, recruits devoted followers, and orchestrates elaborate plans that unfold over months or even years. Yet describing Light as simply “manipulative” does little to explain how he achieves these outcomes. His…
-

What is Obsession About? A Psychological Interpretation of Nikki, Bear, and Attachment
Most interpretations of Obsession focus on the supernatural elements of the story. However, I believe the film’s true horror lies elsewhere. Obsession targets the age-old longing of magical cures to set our insecurities right. The film asks whether one can actually handle the responsibility of a magical cure (the wish) to insecurities surrounding relationships, without…
-
How Cognitive Behavioral Therapy (CBT) Works; Definition, Techniques, Benefits, and Examples
Have you ever noticed how a single thought can completely change your mood? Imagine making a mistake at work and immediately thinking, “I’m terrible at my job.” Within moments, you may feel anxious, discouraged, or even hopeless. You might avoid taking on new responsibilities. Or you could perhaps withdraw from colleagues. Some individuals could also…
-
How Trauma Transformed Light Yagami
Most discussions of Light Yagami focus on his intelligence, narcissism, or eventual god complex (read the main character analysis here). These explanations capture important aspects of his personality, but they often overlook a deeper psychological question: What experiences transformed an exceptionally capable young man into Kira? Contrary to popular belief, Light’s psychological journey is not…
-

What Makes Hannibal Lecter an ENTJ?
Hannibal Lecter’s behavior consistently reflects a preference for external control, structured execution, and the deliberate shaping of outcomes. Rather than remaining a passive observer, Hannibal actively constructs situations that influence others, using his environment very adaptively as a medium through which he imposes order and realizes his intentions. There are two sections of Lecter’s MBTI…
-

Agreeableness Personality Trait
Agreeableness is a personality trait which is associated with being honest, kind, polite, empathatic and coporative and considerate. It is also one of the Big Five personality traits. Curious how agreeable you are compared to the other four traits? You can take our free Big 5 personality test to find out. comprehensively you can define…
-
Eros and Thanatos: Diving into Freud’s Theory of the Life and Death Instincts
Why do people repeat what hurts them, even when they know better? Why does love feel both deeply life-giving and strangely destabilizing? And why do creativity, passion, and self-destruction so often appear side by side in the same person? Sigmund Freud, one of the most influential psychologists and the father of psychoanalysis, tried to answer…
 Psychologus
Psychologus